


- Published on

This week we are doing something a little different. Instead of focusing on one company and their range of offerings, we will instead be looking at carbapenemase-producing organisms. I will cover what they are and why we care about them first, and then show you all of the products we supply for the identification, detection, culture and quality control of CPOs.
The Section about background
What are Carbapenemase-producing organisms (CPOs)?
Carbapenemase-producing organisms are a group of bacteria which produce carbapenemases, making them resistant to the antibiotic, carbapenems. Carbapenems are a beta-lactam antibacterial with a broad spectrum of activity. This spectrum includes many gram-positive and gram-negative bacteria, and anaerobes; imipenem (imipenem with cilastatin) and meropenem have activity against Pseudomonas aeruginosa, but emerging acquired resistance can be a problem. [1]
CPOs can usually be found in the normal gut flora of humans and animals, without causing a problem/ colonising. The issues are apparent when they get into places they are not supposed to be, like the bladder and especially the bloodstream (with a high mortality of 40-50%). This is why it is quite a big issue in hospitals (CPE outbreak 2015/2016) where people are already unwell and on antibiotics, or have a weakened immune system. [2]
[1] https://bnf.nice.org.uk/treatment-summaries/carbapenems/
[2] https://www.uclh.nhs.uk/patients-and-visitors/patient-information-pages/carbapenemase-producing-organisms-cpo
Prevalence and incidence
From October 2020 to December 2024, there were 20 544 reported episodes of acquired carbapenemase-producing organisms (to the UKHSA), with the majority of these being identified from screening samples, accounting for 71.7% of these reports and 910 cases (4.4%) being from sterile sites. However, in Q4 2024 the rate of reported CPO episodes decreased when compared to Q3 2024 (3.3/100 000 population compared to the previous 3.7/100 000 population). This being the highest since mandatory reporting initially began in 2020. [1]
To dive deeper, the highest rate of CPO continued to be in London and the North West (26.2 and 22.7 per 100 000 population, respectively). Furthermore, NHS North West London ICB had the highest rate (40.2 per 100 000 population) and NHS Gloucestershire ICB having the lowest (0.8 per 100 000 population). [1]
Between Q1 2024 and Q4 2024, the most reported acquired carabapenemase was NDM (35.9%), followed up by OXA-48-like (34.4%) and finally KPC (19.6%). This was also seen to vary by region, OXA-48-like was the most reported mechanism in the East of England and the West Midlands, whereas KPC dominated the reports for the North West (NDM being the most reported mechanism throughout). [1]
11 years ago, in 2015, there was a sudden rise in cases of faecal colonisation with KPC-producing E. coli, detected in the Manchester Heart Centre at the Manchester Royal Infirmary. Between the 1st of April 2014 and the 30th of December 2014, there were 23 new CRE-colonised individuals, detected in the MHC, including 2 with E. coli. A CRE outbreak was declared on the 2nd of January 2015, following 6 new CRE-colonised individuals identifications (4 with blaKPC and 2 with blaNDM; no E. coli). [2]
Following the outbreak, investigations identified that the bacteria were present in clinical hand-wash basins, sink sites and floor scrubbers. This lead to the trust implementing strict environmental cleaning, enhanced surveillance for patients, and routine screening of patients. By January 2015, the Manchester foundation trust were operating a trust-wide screening program (>110 screens/day). From September-December 2014, 16 612 samples from 7 239 inpatients were screened using either culture (9 808 samples), or PCR and culture (6 804). Overall, CRE prevalence was 3.8% (438 positive samples from 272 patients), with molecular mechanism data for 135/163 PCR-positive samples indicating that blaKPC accounted for most carbapenem resistance (97%). [2]
[1] https://www.gov.uk/government/publications/carbapenemase-producing-gram-negative-bacteria-laboratory-surveillance/carbapenemase-producing-gram-negative-organisms-in-england-since-october-2020-quarterly-update-q4-2024#background
[2] https://pmc.ncbi.nlm.nih.gov/articles/PMC6256751/
Carbapenemase-producing organisms are a group of bacteria which produce carbapenemases, making them resistant to the antibiotic, carbapenems. Carbapenems are a beta-lactam antibacterial with a broad spectrum of activity. This spectrum includes many gram-positive and gram-negative bacteria, and anaerobes; imipenem (imipenem with cilastatin) and meropenem have activity against Pseudomonas aeruginosa, but emerging acquired resistance can be a problem. [1]
CPOs can usually be found in the normal gut flora of humans and animals, without causing a problem/ colonising. The issues are apparent when they get into places they are not supposed to be, like the bladder and especially the bloodstream (with a high mortality of 40-50%). This is why it is quite a big issue in hospitals (CPE outbreak 2015/2016) where people are already unwell and on antibiotics, or have a weakened immune system. [2]
[1] https://bnf.nice.org.uk/treatment-summaries/carbapenems/
[2] https://www.uclh.nhs.uk/patients-and-visitors/patient-information-pages/carbapenemase-producing-organisms-cpo
Prevalence and incidence
From October 2020 to December 2024, there were 20 544 reported episodes of acquired carbapenemase-producing organisms (to the UKHSA), with the majority of these being identified from screening samples, accounting for 71.7% of these reports and 910 cases (4.4%) being from sterile sites. However, in Q4 2024 the rate of reported CPO episodes decreased when compared to Q3 2024 (3.3/100 000 population compared to the previous 3.7/100 000 population). This being the highest since mandatory reporting initially began in 2020. [1]
To dive deeper, the highest rate of CPO continued to be in London and the North West (26.2 and 22.7 per 100 000 population, respectively). Furthermore, NHS North West London ICB had the highest rate (40.2 per 100 000 population) and NHS Gloucestershire ICB having the lowest (0.8 per 100 000 population). [1]
Between Q1 2024 and Q4 2024, the most reported acquired carabapenemase was NDM (35.9%), followed up by OXA-48-like (34.4%) and finally KPC (19.6%). This was also seen to vary by region, OXA-48-like was the most reported mechanism in the East of England and the West Midlands, whereas KPC dominated the reports for the North West (NDM being the most reported mechanism throughout). [1]
11 years ago, in 2015, there was a sudden rise in cases of faecal colonisation with KPC-producing E. coli, detected in the Manchester Heart Centre at the Manchester Royal Infirmary. Between the 1st of April 2014 and the 30th of December 2014, there were 23 new CRE-colonised individuals, detected in the MHC, including 2 with E. coli. A CRE outbreak was declared on the 2nd of January 2015, following 6 new CRE-colonised individuals identifications (4 with blaKPC and 2 with blaNDM; no E. coli). [2]
Following the outbreak, investigations identified that the bacteria were present in clinical hand-wash basins, sink sites and floor scrubbers. This lead to the trust implementing strict environmental cleaning, enhanced surveillance for patients, and routine screening of patients. By January 2015, the Manchester foundation trust were operating a trust-wide screening program (>110 screens/day). From September-December 2014, 16 612 samples from 7 239 inpatients were screened using either culture (9 808 samples), or PCR and culture (6 804). Overall, CRE prevalence was 3.8% (438 positive samples from 272 patients), with molecular mechanism data for 135/163 PCR-positive samples indicating that blaKPC accounted for most carbapenem resistance (97%). [2]
[1] https://www.gov.uk/government/publications/carbapenemase-producing-gram-negative-bacteria-laboratory-surveillance/carbapenemase-producing-gram-negative-organisms-in-england-since-october-2020-quarterly-update-q4-2024#background
[2] https://pmc.ncbi.nlm.nih.gov/articles/PMC6256751/

First up, we have CHROMagar Microbiology and their mSuperCARBA dehydrated media for the detection of a wide range of carbapenemase producers (OXA, NDM, VIM, IMP, KPC).
CHROMagar mSuperCARBA was designed to simplify the detection of CPEs, including the big five (OKNVI), this allows for the improved monitoring of high-risk patients and routine screening of inpatients and transfers. The distinctive colours produced by individual colonies allows for the presumptive positive results to be assessed within 24hrs of reception of the sample.
What more can I say? It's dehydrated media that you can sit on your shelf in your storeroom, it has a shelf life of almost 2 years so you'll never go to use it to find it's gone out of date. You just pour the plates when you need them, in the exact quantity you need them. 5L of dehydrated media will make about 250 plates too!
CHROMagar mSuperCARBA was designed to simplify the detection of CPEs, including the big five (OKNVI), this allows for the improved monitoring of high-risk patients and routine screening of inpatients and transfers. The distinctive colours produced by individual colonies allows for the presumptive positive results to be assessed within 24hrs of reception of the sample.
What more can I say? It's dehydrated media that you can sit on your shelf in your storeroom, it has a shelf life of almost 2 years so you'll never go to use it to find it's gone out of date. You just pour the plates when you need them, in the exact quantity you need them. 5L of dehydrated media will make about 250 plates too!

Next up, we have Rosco Diagnostica and their diagnostic kits. There are two main kits we'll be looking at, these being the KPC, MBL & OXA-48 confirm kit, and the KPC and MBL confirm kit (in Pseudomonas aeruginosa and Acinetobacter)
Rosco Diagnostica has developed and produces convenient systems for the detection, rapid colorimetric and assembled kits with disc diffusion tablets, complete with ready-to-use cartridges of the necessary combined Neo-Sensitabs or Diatabs, and a guide to their use. Rosco diagnostica rapid colorimetric kits have the following advantages over their competitors:
Rosco Diagnostica has developed and produces convenient systems for the detection, rapid colorimetric and assembled kits with disc diffusion tablets, complete with ready-to-use cartridges of the necessary combined Neo-Sensitabs or Diatabs, and a guide to their use. Rosco diagnostica rapid colorimetric kits have the following advantages over their competitors:
- No reagent preparation needed
- Longer shelf-life, most Neo-sensitabs do NOT need refrigeration, and the ones that do can remain on a bench out of the fridge for 2 months during use!
- Stable crystalline imipenem.
- Lower cost
Microbiologics have quite a few different products for CPOs, ranging from KWIK-STIKs for you OKNVI's, individual ATCC accredited organisms, and molecular diagnostic quality controls.
Helix Elite molecular standards are advanced quality control materials designed to support the development, validation, and routine monitoring of molecular diagnostic assays. Used across PCR and other nucleic acid-based technologies, these controls help laboratories across the UK and US ensure accuracy, detect visibility, and maintain confidence in test results while meeting regulatory requirements. For Carabpenem-resistant Enterobacteriaceae, there is one control panel, this being: #8187 Carbapenem-resistant Enterobacteriaceae (CRE) Control Panel (Inactivated swab). This kit includes 6 positive control swabs and 6 negative control swabs. Each positive swab consisting of:
For your OKNVI's (OXA, KPC, NDM, VIM, IMP) there are individual organisms that can be used for your phenotyping and quality controls. These being:
Helix Elite molecular standards are advanced quality control materials designed to support the development, validation, and routine monitoring of molecular diagnostic assays. Used across PCR and other nucleic acid-based technologies, these controls help laboratories across the UK and US ensure accuracy, detect visibility, and maintain confidence in test results while meeting regulatory requirements. For Carabpenem-resistant Enterobacteriaceae, there is one control panel, this being: #8187 Carbapenem-resistant Enterobacteriaceae (CRE) Control Panel (Inactivated swab). This kit includes 6 positive control swabs and 6 negative control swabs. Each positive swab consisting of:
- Escherichia coli derived from NCTC 13476
- Klebsiella pneumoniae derived from NCTC 13440
- Klebsiella pneumoniae derived from NCTC 13443
- Klebsiella pneumoniae derived from NCTC 13438
- Klebsiella pneumoniae derived from NCTC 13442
For your OKNVI's (OXA, KPC, NDM, VIM, IMP) there are individual organisms that can be used for your phenotyping and quality controls. These being:
- OXA: #01148P - Klebsiella pneumoniae derived from NCTC 13442
- KPC: #01117P - Klebsiella pneumoniae derived from NCTC 13438
- NDM: #01060P - Klebsiella pneumoniae derived from ATCC BAA-2146*
- VIM: #01112P - Klebsiella pneumoniae derived from NCTC 13440
- IMP - #01136P - Escherichia coli derived from NCTC 13476
Finally, we have AmplexDiagnostics GmbH and their SuperBug series for the detection of various carbapenemase producers via real-time PCR. The eazyplex SuperBug CRE assay can be a useful tool for a rapid (less than 20 mins) and reliable identification of resistance mechanism genes in Gram-negative rods, and also directly from urine and pre-cultured blood samples.
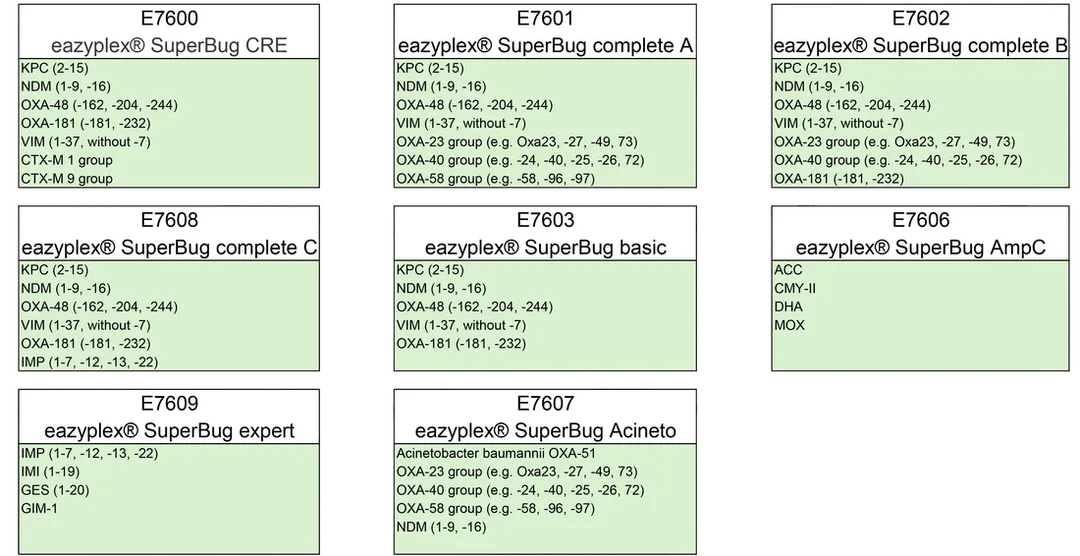
These rapid diagnostic tests cover both prevalent Gram-negative resistances (such as KPC, NDM, and CTX-M) and the less prevalent, but equally important, resistance genes such as GIM, GES, and AmpC.
The eazyPlex SuperBug series is a molecular identification product based on LAMP technology, with key features such as:
The eazyPlex SuperBug series is a molecular identification product based on LAMP technology, with key features such as:
- Turn-around-times under 30 minutes
- Ease of use, no DNA extraction
- Suitable for single or small numbers of tests
- Samples from urine, rectal swab, blood culture and agar plates
- High accuracy
I am once again done yapping for this week, I hope you enjoyed this post on Carbapenem-resistance and all that.
0 Comments
