
- Published on
Welcome! Welcome!
We're back this week to talk about SensID and their genomic reference material! SensID are a Microbiologics company, specialising in the development & manufacturing of reference material and quality controls in DNA diagnostics.
They produce a range of products such as reference materials/ quality controls which are precisely characterised and manufactured under the highest standards.
SensID's products are an ideal solution for R&D, the validation of instruments, for use as an external control, in the preparation for accreditation, ring trials, conformity assessments, as part of a diagnostic test kit, and more!
In May 2024, SensID launched their metagenome control material, promising to revolutionise molecular healthcare through the rapid identification of thousands of microbes. The control material enables the detection of bacteria, DNA viruses, fungi and parasite all within a single day using next-generation sequencing and polymerase chain reaction platforms
This product is ideally suited for Next Generation Sequencing (NGS) workflows. Especially for:
- Assay validation. This means that it can be used as a spike-in reference to confirm that the extraction, library preparation, and sequencing pipelines accurately detect low-abundance microbial DNA without high background interference.
- Pipeline comparison. Datasets curated from SensID standards can be compared to bioinformatics tools to optimise pathogen detection algorithms (such as distinguishing true microbial presence from wet-lab contamination).
Sensid's full catalogue
Sensid's full catalogue
SensID don't just have cfDNA in Plasma for Metagenomics, they have a whole range of genomic reference material for whatever you may need. For more information on SensID's product range please use the link!
Product Brochure
Product Brochure
We also have a product brochure with lots of information in it, it's the same one we give out at events & conferences, so if you would like a copy we can send you one too!


Heading
While stocks last, we are giving out complimentary samples of the Mini FPC system by REAL. If you would like more information, or to request your complimentary sample, reach out to us using the link!
REAL's mini FPC system is ideal for people who don't want the faff of formaldehyde, whilst maintaining the same fixing power.
- Published on
Welcome! Welcome!
Welcome back to your regularly (not really) scheduled program of me telling you about something!
This week is a new week! which means we're talking about a new company: ERA Biology! These folks have a range of different products, ranging from lateral flow assays, to real-time PCR, to machines that do the reading for you!
ERa's Catalogue
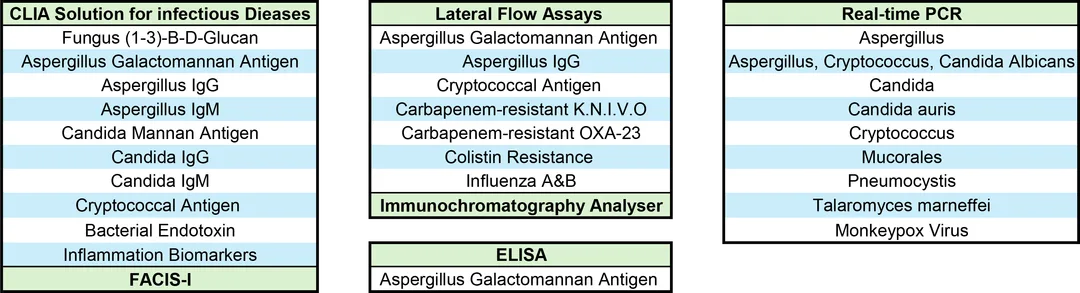
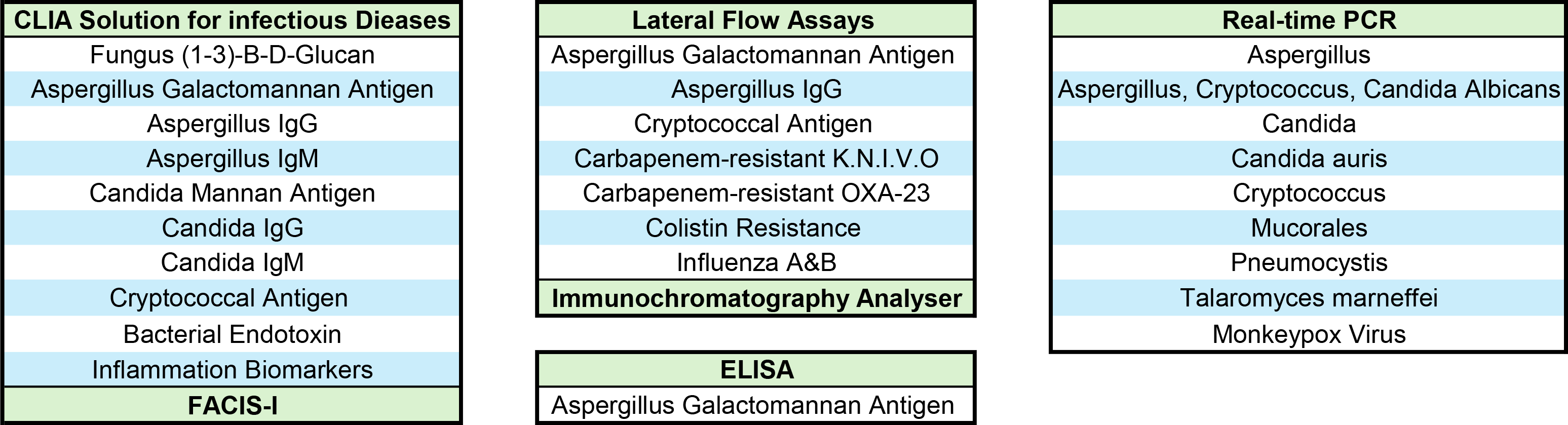
Here's a table for you! I have collected all of the tests together, so you have a nice easy viewing experience finding out if ERA do a test you're interested in. You're welcome!
Fungixpert Lateral flow assays
Fungixpert Lateral flow assays
The FungiXpert range is a range of lateral flow assays for use in fungal diagnostics for the rapid detection of the most common fungal pathogens.
The Lateral flow product range includes:
-
Aspergillus Galactomannan
-
Aspergillus IgG
-
Aspergillus IgM
-
Candida Mannan
-
Candida IgG
-
Candida IgM
-
Cryptococcal Capsular Polysaccharide
The LFA Reader
The LFA Reader
The Immunochromatography analyser is a pre-programmed instrument, for the quantitative reading of lateral flow assays.
It is compatible with a range of lateral flow tests from the FungiXpert range.

The immunochromatography reader is a pre-programmed instrument for quantitatively reading lateral flow assays. The reader itself has a built-in standard curve, which is recognised by the ID on the cassette itself.
Boasting simple operation, where the barcode for the test is scanned, read and results presented by the handheld device. The quantitative results are displayed as determined by the barcode detected standard curve.

The FACIS MAchine
The FACIS MAchine
ERA's solution for real-time PCR fungal diagnostics.
Sporting features such as:
- Special Sample pretreatment systems
- Independent reagent cartridges
- Fully automatic proccesses
The FACIS machine revolutionises fungal diagnostics, being simple, rapid and suitable for all laboratories.
The FACIS is an open system used to detect the content of endotoxins, (1-3)-B-D-glucan and galactomannan in human BAL fluid, or serum, samples. With both photometry, and chemilluminscence systems built in.
In addition to this, the FACIS machine also provides rapid and reliable results for over 10 tests that use CLIA, or chromogenic methods, including but not limited to: bacterial endotoxin test, candida mannan test, interleukin & CRP.
- Published on


welcome! welcome!
This week (and whilst stocks last) we are giving away a free sample of the Mini FPC System with Total-Fix to anyone who wants to try it out. It's as free as it comes and available until we literally run out of them to give away so do not hesitate to reach out to us, we will send you one!
GET YOUR FREE POO KIT!
GET YOUR FREE POO KIT!
If you would like a free sample of the Mini FPC system, please reach out to us and we will send you a free sample, it's completely free so you have nothing to lose.
REAL by Durviz
Now you may remember I've spoken about these folks before, so If you remember what I said last time, great! If you've never heard of them before, let me tell you all about them.
REAL is a specialised brand of laboratory analysis and life-science products owned by Durviz S.L. which is a biotechnology company based in Valencia, Spain. The REAL product range focuses specifically on molecular biology, parasitology, and clinical sample collections, with their primary offerings including:
- The innovative Mini and Midi systems, which are closed, clean & ecological collection devices designed to safely store and concentrate stool samples for intestinal parasite and helminth egg detection.
- The Graham Test, a ready to use, glass slide with adhesive tape, for the diagnosis of the presence of pinworm eggs in the perianal area. It is designed to be safe and easy to use, simplifying the sampling process by avoiding patient contact with glass and contamination through direct contact with the perianal area.
The Mini and Midi FPC System
The REAL Mini & Midi system is a patented device for stool sample conservation and concentration, it is "the best solution for your laboratory to manage faecal samples. Being cleaner, smaller, more effective and ecological."
The system is designed to simplify sample processing, with no additional consumables being required. The long spoon ensures the technician is not in touch with the sample at anytime, keeping them protected from touching the sample, whilst the fixative turns the sample non-infective. Furthermore, the inclusion of glass beads in the sample chamber benefit with the homogenisation of the sample.
More information? I thought you'd never ask:
- Cap with tablespoon and glass beads for homogenisation
- Small amount of sample required
- Sedimentation cone for centrifugation
- Compatible with 15ml/50ml centrifuge rotors
- Plastic bag for the transport of the samples and clinical data sheet
- Four-step procedure
- Two different filters (400 and 250 microns) to separate the debris in the sample from the specimen without clogging
- 4ml or 10ml of fixative respectively
- Caps available for sediment storage (optional)
- EASYPICK (Optional): Pipettes and pierced caps for a clean collection of the sediment
- Tube rack, for easy handling and management
- Special silicone seals to prevent leakages
- CE IVD Marked.
Formaldehyde is not scary when you don't use it
The Mini and Midi systems come pre-loaded with Total-fix fixative. What makes this special is that it is Formaldehyde, mercury and PVA free, boasting the same fixing power as that of Formaldehyde based fixatives.
Furthermore, as Total-fix is not Formaldehyde based, that means that the same sample is also compatible with molecular techniques, without the need for a separate sample. Now if Total-Fix doesn't sound like your cup of tea, we also supply the Mini and Midi empty, with no fixative included so you can use your own.
Did I mention we're giving stuff away? For free!
Yes if you missed it earlier I will re-iterate it, we are giving away a sample of the Mini FPC system, with Total-Fix included, for free! No strings attached, on the house, complimentary, as a bonus. You name it we'll give it to you for free!
This is only available while we have it in stock, when we run out, we run out and we go back to charging you for it. If you would like your sample, reach out to us at: welcome@bioconnections.co.uk or give us a call on: 01782 516010.
- Published on
WELCOME! WELCOME!
That's right we're back, returning from our may hiatus (I was too busy organising and redesigning the catalogue page) to talk to you about Microbiologics' range of multiplex QC panels for Cepheid GeneXpert and the BioFire film array panels.
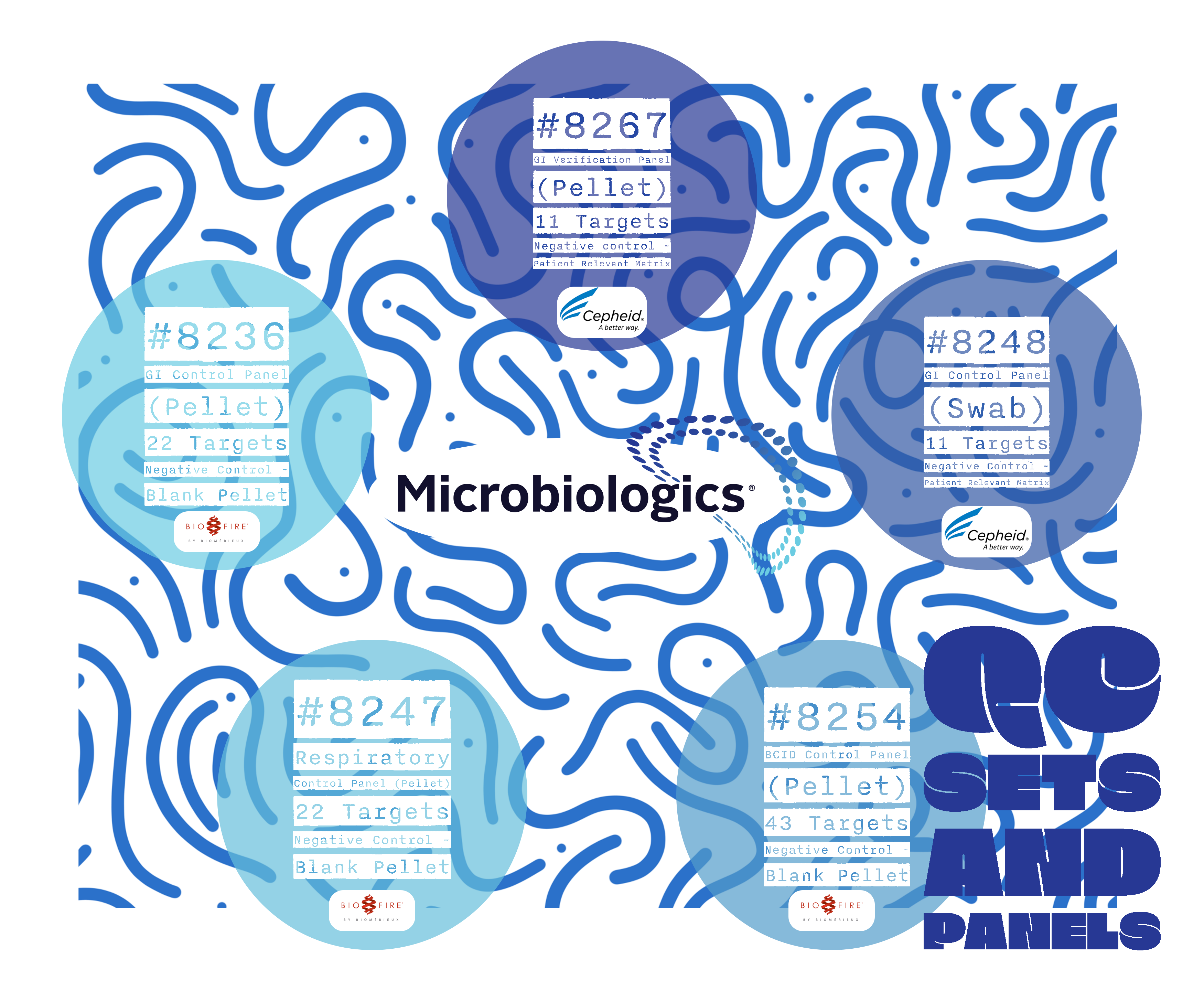
As you can see, we're talking about five specific panels that have a range of targets and are intended for use with specific panels and instruments. To break it down for you:
For the Cepheid Xpert GI Panel:
- #8267: GI Verification Panel (Pellet) - 11 Targets. Negative Control - Patient relevant matrix.
- #8248: GI Control Panel (Swab) - 11 Targets. Negative Control - Patient relevant matrix.
For the BioFire BCID2 Panel:
- #8254: BCID Control Panel (Pellet) - 43 Targets. Negative Control - Blank pellet.
For the BioFire respiratory 2.1 Panel:
- #8247: Respiratory Control Panel (Pellet) - 22 Targets. Negative Control - Blank Pellet.
For the BioFire Gastrointestinal panel:
- #8236: GI Control Panel (Pellet) - 22 Targets. Negative Control - Blank pellet.

System-Specific Panels
System-Specific Panels
For more information of the specific targets of each panel, please follow this link
Why you should use third-party controls in your lab
Within clinical laboratories, it is important to ascertain and maintain the highest possible standards of accuracy and reliability in test performance.
Therefore, routine internal quality control checks are integral to this process and are performed daily, sometimes multiple times per day, weekly or monthly.
This routine QC ensures the precision and reliability of both analytical instruments and their reagents. Some key benefits to using third-party controls are as follows:
- They allow for the independent and unbiased assessment of instruments and method performance.
- They are highly consolidated QC materials, this means that the laboratory can save time, space and costs by combining multiple controls into a single, efficient solution.
- Compliance with ISO 15189 is a point that is always spoken about, especially when UKAS visits are incoming. The use of third-party QCs helps laboratories meet these stringent regulatory and accreditation requirements, ensuring high standards of practice.


So why choose Microbiologics?
In their own words, Microbiologics "maximises the advantages of external controls by engineering QC products to resemble patient samples in the manner of sample collection and handling".
Their controls are available as lyophilised swab and pellet formats, with their molecular controls designed to be processed as if they were patient samples. They have a vast portfolio for the KWIK-STIKs alone, including the major syndromic groups of infectious disease. Chances are if you are looking for a control, whether it's syndrome, or system, specific, Microbiologics have a control for it.
- Published on
It's a new week, so it's a new BioConnections post! This week we're talking blood culture identification (BCID). BCID is covered mainly by Microbiologics and their QC panels, but you'll never guess what! We supply our own Fastidious Anaerobe Agar (F.A.A) for culturing your positive blood cultures on!
Blood Culture Identification
Complementing this, BioConnections (our own) FAA Agar provides a high-performance medium for the cultivation of fastidious anaerobes, supporting consistent growth and reproducible results. Together, these tools empower laboratories to maintain the highest standards in microbiological testing while enhancing efficiency and patient outcomes.
Microbiologics

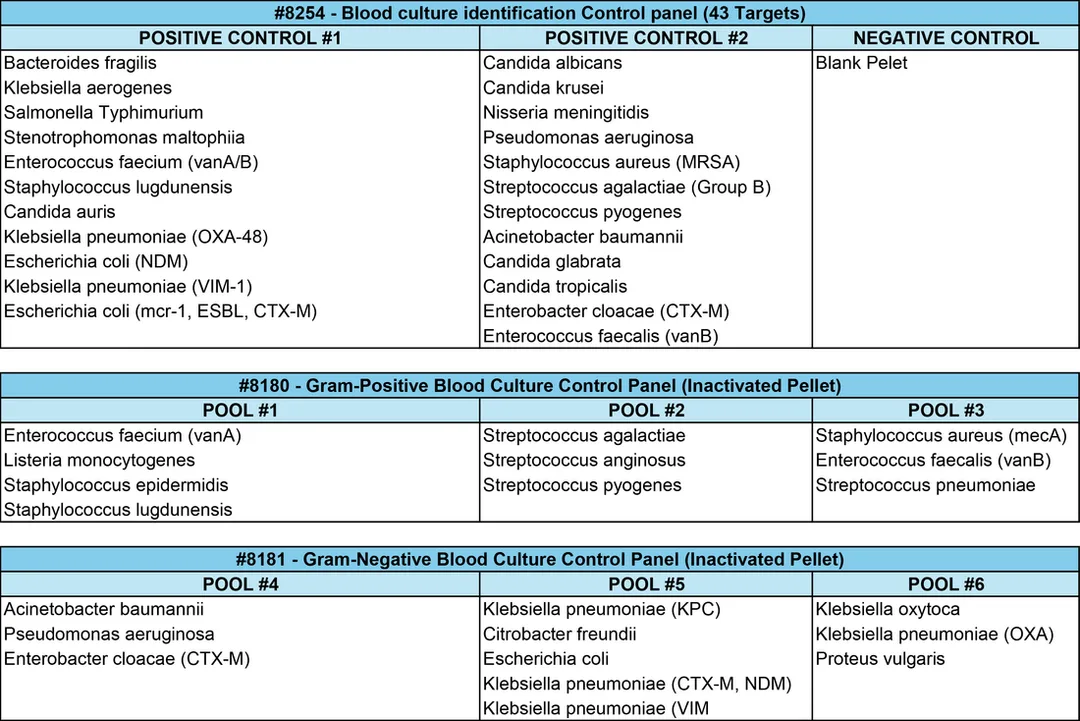
The Gram-Negative Blood Culture Control Panel also includes 3 pools containing 3-5 inactivated microorganisms per pool. Kits contain 5 vials of each pool (15 total vials) and feature colour coordinated labels for easy pool identification.
BioConnections
Yes your eyes are working correctly, We offer our own F.A.A agar for you to pour your own plates. These plates have one of the same benefits as CHROMagar dehydrated media (if you think back to last week), it has a super long shelf-life! It comes in either 500g or 2.5kg that can be sent to you!

Our medium also has the option to be made selective with the addition of antibiotic supplements. This is the medium of choice for the routine isolation of clinically significant anaerobes, our medium supports the growth of most fastidious anaerobes. Classical colony formation, odour and fluorescence under UV are diagnostic features on this medium. The choice of peptones and growth factors provide early growth of most organisms whilst the starch has an important role as a de-toxification agent. The medium is often made selective for various groups of anaerobes by the addition of appropriate selective agents.
- Published on

The Section about background
Carbapenemase-producing organisms are a group of bacteria which produce carbapenemases, making them resistant to the antibiotic, carbapenems. Carbapenems are a beta-lactam antibacterial with a broad spectrum of activity. This spectrum includes many gram-positive and gram-negative bacteria, and anaerobes; imipenem (imipenem with cilastatin) and meropenem have activity against Pseudomonas aeruginosa, but emerging acquired resistance can be a problem. [1]
CPOs can usually be found in the normal gut flora of humans and animals, without causing a problem/ colonising. The issues are apparent when they get into places they are not supposed to be, like the bladder and especially the bloodstream (with a high mortality of 40-50%). This is why it is quite a big issue in hospitals (CPE outbreak 2015/2016) where people are already unwell and on antibiotics, or have a weakened immune system. [2]
[1] https://bnf.nice.org.uk/treatment-summaries/carbapenems/
[2] https://www.uclh.nhs.uk/patients-and-visitors/patient-information-pages/carbapenemase-producing-organisms-cpo
Prevalence and incidence
From October 2020 to December 2024, there were 20 544 reported episodes of acquired carbapenemase-producing organisms (to the UKHSA), with the majority of these being identified from screening samples, accounting for 71.7% of these reports and 910 cases (4.4%) being from sterile sites. However, in Q4 2024 the rate of reported CPO episodes decreased when compared to Q3 2024 (3.3/100 000 population compared to the previous 3.7/100 000 population). This being the highest since mandatory reporting initially began in 2020. [1]
To dive deeper, the highest rate of CPO continued to be in London and the North West (26.2 and 22.7 per 100 000 population, respectively). Furthermore, NHS North West London ICB had the highest rate (40.2 per 100 000 population) and NHS Gloucestershire ICB having the lowest (0.8 per 100 000 population). [1]
Between Q1 2024 and Q4 2024, the most reported acquired carabapenemase was NDM (35.9%), followed up by OXA-48-like (34.4%) and finally KPC (19.6%). This was also seen to vary by region, OXA-48-like was the most reported mechanism in the East of England and the West Midlands, whereas KPC dominated the reports for the North West (NDM being the most reported mechanism throughout). [1]
11 years ago, in 2015, there was a sudden rise in cases of faecal colonisation with KPC-producing E. coli, detected in the Manchester Heart Centre at the Manchester Royal Infirmary. Between the 1st of April 2014 and the 30th of December 2014, there were 23 new CRE-colonised individuals, detected in the MHC, including 2 with E. coli. A CRE outbreak was declared on the 2nd of January 2015, following 6 new CRE-colonised individuals identifications (4 with blaKPC and 2 with blaNDM; no E. coli). [2]
Following the outbreak, investigations identified that the bacteria were present in clinical hand-wash basins, sink sites and floor scrubbers. This lead to the trust implementing strict environmental cleaning, enhanced surveillance for patients, and routine screening of patients. By January 2015, the Manchester foundation trust were operating a trust-wide screening program (>110 screens/day). From September-December 2014, 16 612 samples from 7 239 inpatients were screened using either culture (9 808 samples), or PCR and culture (6 804). Overall, CRE prevalence was 3.8% (438 positive samples from 272 patients), with molecular mechanism data for 135/163 PCR-positive samples indicating that blaKPC accounted for most carbapenem resistance (97%). [2]
[1] https://www.gov.uk/government/publications/carbapenemase-producing-gram-negative-bacteria-laboratory-surveillance/carbapenemase-producing-gram-negative-organisms-in-england-since-october-2020-quarterly-update-q4-2024#background
[2] https://pmc.ncbi.nlm.nih.gov/articles/PMC6256751/

CHROMagar mSuperCARBA was designed to simplify the detection of CPEs, including the big five (OKNVI), this allows for the improved monitoring of high-risk patients and routine screening of inpatients and transfers. The distinctive colours produced by individual colonies allows for the presumptive positive results to be assessed within 24hrs of reception of the sample.
What more can I say? It's dehydrated media that you can sit on your shelf in your storeroom, it has a shelf life of almost 2 years so you'll never go to use it to find it's gone out of date. You just pour the plates when you need them, in the exact quantity you need them. 5L of dehydrated media will make about 250 plates too!

Rosco Diagnostica has developed and produces convenient systems for the detection, rapid colorimetric and assembled kits with disc diffusion tablets, complete with ready-to-use cartridges of the necessary combined Neo-Sensitabs or Diatabs, and a guide to their use. Rosco diagnostica rapid colorimetric kits have the following advantages over their competitors:
- No reagent preparation needed
- Longer shelf-life, most Neo-sensitabs do NOT need refrigeration, and the ones that do can remain on a bench out of the fridge for 2 months during use!
- Stable crystalline imipenem.
- Lower cost
Helix Elite molecular standards are advanced quality control materials designed to support the development, validation, and routine monitoring of molecular diagnostic assays. Used across PCR and other nucleic acid-based technologies, these controls help laboratories across the UK and US ensure accuracy, detect visibility, and maintain confidence in test results while meeting regulatory requirements. For Carabpenem-resistant Enterobacteriaceae, there is one control panel, this being: #8187 Carbapenem-resistant Enterobacteriaceae (CRE) Control Panel (Inactivated swab). This kit includes 6 positive control swabs and 6 negative control swabs. Each positive swab consisting of:
- Escherichia coli derived from NCTC 13476
- Klebsiella pneumoniae derived from NCTC 13440
- Klebsiella pneumoniae derived from NCTC 13443
- Klebsiella pneumoniae derived from NCTC 13438
- Klebsiella pneumoniae derived from NCTC 13442
For your OKNVI's (OXA, KPC, NDM, VIM, IMP) there are individual organisms that can be used for your phenotyping and quality controls. These being:
- OXA: #01148P - Klebsiella pneumoniae derived from NCTC 13442
- KPC: #01117P - Klebsiella pneumoniae derived from NCTC 13438
- NDM: #01060P - Klebsiella pneumoniae derived from ATCC BAA-2146*
- VIM: #01112P - Klebsiella pneumoniae derived from NCTC 13440
- IMP - #01136P - Escherichia coli derived from NCTC 13476
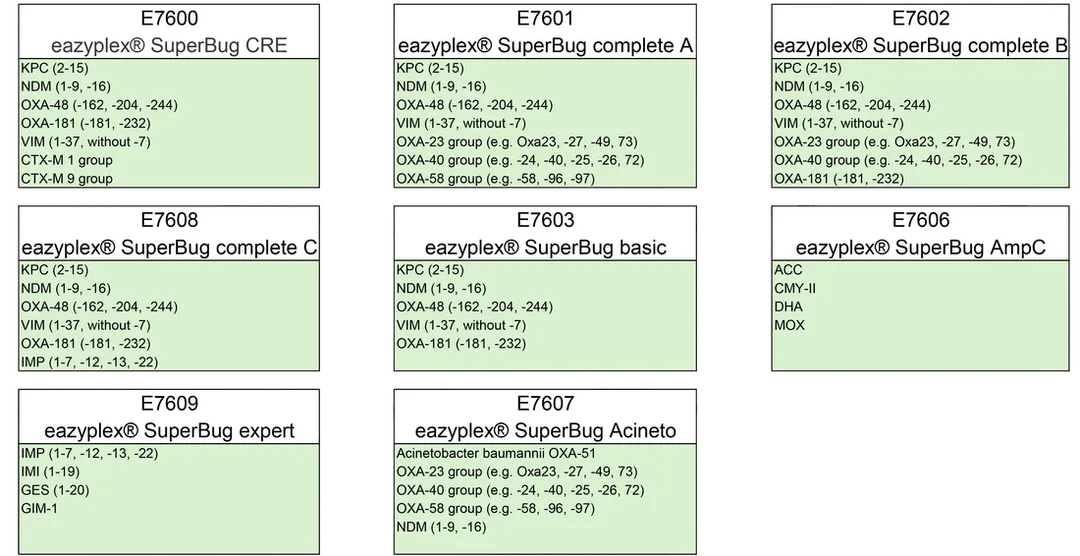
The eazyPlex SuperBug series is a molecular identification product based on LAMP technology, with key features such as:
- Turn-around-times under 30 minutes
- Ease of use, no DNA extraction
- Suitable for single or small numbers of tests
- Samples from urine, rectal swab, blood culture and agar plates
- High accuracy
- Published on
For the un-initiated, I will include a bit of information about what chromogenic media is and why it's neat so don't worry if you've never heard of a CHROMagar!
What we're talking about today is a little different to how you might know CHROMagar, as we instead deal with their plates in powder form! Now you may think this is pretty old-school, BUT!, there are benefits to dehydrated media compared to your usual fridge-stored plates.


What are chromogenic media plates?
Chromogenic materials are defined as substances that exhibit a reversible change in coloration, in response to external stimuli. Chromogenic media contains chromogens, consisting of a substrate and a chromophore. Plates, before use are colourless because the chromophore does not absorb visible light whilst conjugated to the substrate [1].
When a specific bacterial organisms enzymatic activity comes into contact with the chromogen molecule, that enzyme cleaves the chromogen molecule which releases the chromophore, as this chromophore is no longer conjugated, the light becomes visible [1].
The chromophore used does not diffuse readily into the surrounding media, meaning that the colour stays concentrated in the area specifically where the bacterial colony with the target enzymatic activity grew. This is why the colony itself takes on the chromophores colour [1].
Chromogenic media utilise synthetic chromogenic enzyme substrates in order to specifically target pathogenic species, based on their enzyme activity. This enzyme activity is never completely species-specific, requiring the use of complementary enzyme substrates and/ or selective agents. This means that the majority of chromogenic media are both selective and differential as they accommodate the inhibition of non-target organisms whilst enabling target pathogens to grow as coloured colonies due to their metabolism, which is usually through hydrolysis, of one or more chromogenic enzyme substrates [2].
[1] https://asm.org/articles/2020/september/how-chromagar-tm-revolutionized-bacterial-identifi
[2] https://pmc.ncbi.nlm.nih.gov/articles/PMC5355637/
What CHROMagar plates are there?
For more information on each specific product, and to speak with us about these chromogenic plates, visit our CHROMagar website at: https://www.bioconnections.co.uk/chromagar-home.html.

Cherry Picking
CHROMagar ESBL
CHROMagar mSuperCARBA
CHROMagar MRSA
CHROMagar Acinetobacter
CHROMagar COL-APSE
CHROMagar LIN-R
The power of powder

- Dehydrated media has a much longer shelf-life, instead of a month or two (I think that's the norm for pre-poured media) this stuff LASTS, you can see in the above photo, this bottle of CHROMagar mSuperCARBA does't expire for YEARS.
- So, these bottles are from 5L to 25L, and with 5L (pouring at 20mL per plate) that will make somewhere in the range of 250 plates. Which is quite a lot for how much space it takes up (not as much as your box of 200 plates that needs to go in the fridge).
Now, I am not saying dehydrated media is better than pre-poured plates, as it just isn't as convenient as grabbing the plates out the fridge when you need them. But think of the times where you have to bin expired media that just didn't get used. Especially with the lesser-used highly selective (expensive) media, with dehydrated media, you could always have it in stock, and you could make up only what you need when you need it, reducing waste and lost money.
Okay I'm done talking now, you can check out CHROmagar if you want! I think they're pretty neat.
- Published on
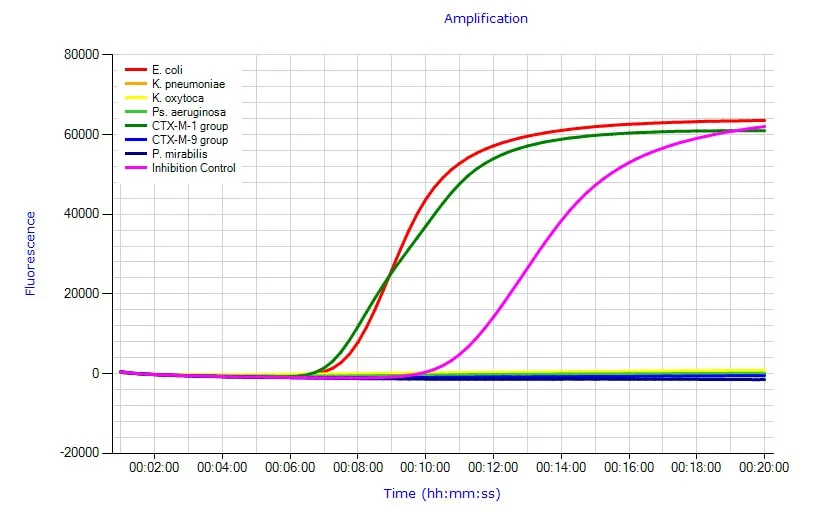
The examination is carried out directly from the positive blood culture without DNA extraction within 20 minutes.
Antimicrobial resistance is a key factor determining clinical unresponsiveness to treatment and rapid progression in sepsis and septic shock.
Details
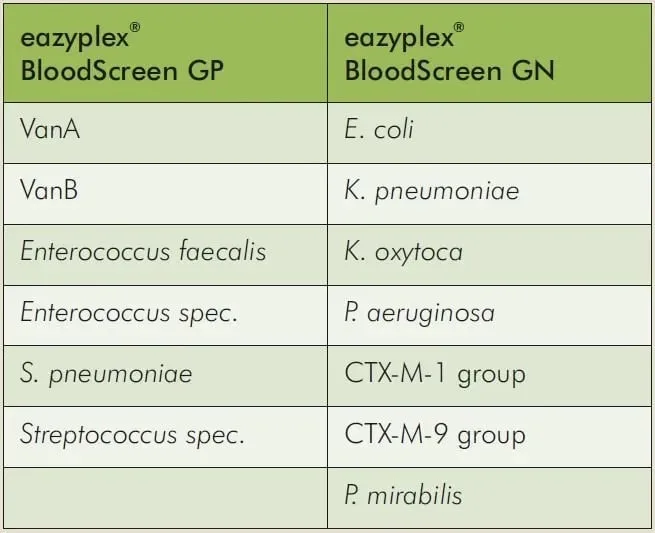
The most common parameters are available to you with the eazyplex® BloodScreen Panels for the Gram positive and the Gram negative spectrum. The examination is carried out directly from the positive blood culture without DNA extraction.
- Hands-on-time approx. 3 min.
- First signals in less than 10 min.
- Complete test run finished in 20 min.
- Results output as PDF, CSV and adhesive label
Evaluations
Performance of the eazyplex® BloodScreen GN as a simple and rapid molecular test for identification of Gram-negative bacteria from positive blood cultures
Eur J Clin Microbiol Infect Dis . 2022 Mar;41(3):489-494. doi: 10.1007/s10096-021-04383-3.
'A total of 449 BCs were analyzed.
Sensitivities and specificities were 100% and 100% for Escherichia coli, 95.7% and 100% for Klebsiella pneumoniae, 100% and 100% for blaCTX-M, 100% and 100% for Klebsiella oxytoca, 100% and 99% for Proteus mirabilis, and 100% and 99.8% for Pseudomonas aeruginosa, respectively.
The time to result ranged from 8 to 16 min, plus about 6 min for sample preparation. The eazyplex® BloodScreen GN is a reliable molecular assay for rapid BC testing.'

A modest investment in one of our Amplex LAMP instruments opens the door
to reducing TATs for key infections.
All our LAMP assays can be used with all our instruments.
Reduce TATs for a wide range of key infections.
The eazyplex® BloodScreen products have these features in common.
Easy to use and portable system
Isothermal Amplification
Testing directly from positive blood culture
Real-time detection in < 30 minutes
Lyophilised reagents
