The graphics below are representations of 3 important aspects of CoVID-19 infections.
- The infection timeline from pre-symptomatic to critical illness with reference to antibody production
- Infection rate relating the samples sent to the laboratory to the progress of infection and it's impact 'sensitivity' of product evaluations
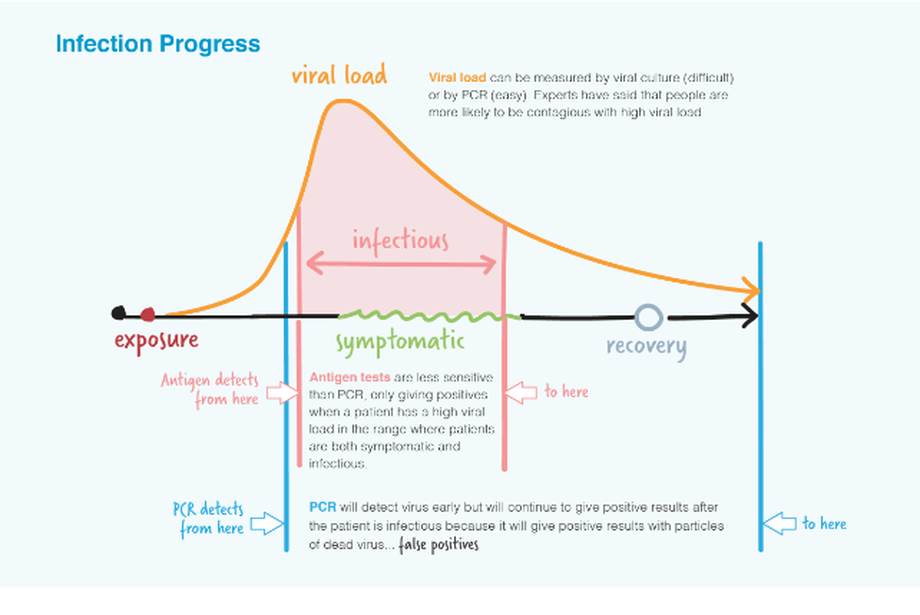
- The third graphic compares the viral load detection range for PCR and Antigen tests and highlights the implications
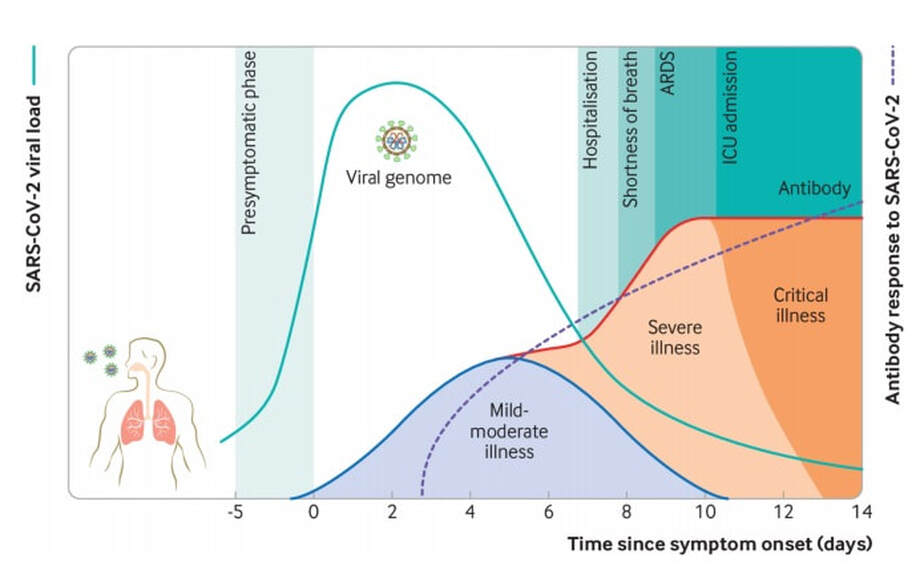
In the respiratory tract, peak SARS-CoV-2 load is observed at the time of symptom onset or in the first week of illness, with subsequent decline, thereafter, indicating the highest infectious potential just before or within the first five days of symptom onset.
(RT-PCR) tests can detect viral SARS-CoV-2 RNA in the upper respiratory tract for a mean of 17 days: however, detection of viral RNA does not necessarily equate to infectiousness and viral culture has been rarely positive beyond nine days of illness.
reference
BMJ 2020;371:m3862 http://dx.doi.org/10.1136/bmj.m3862 Published: 23 October 2020
(RT-PCR) tests can detect viral SARS-CoV-2 RNA in the upper respiratory tract for a mean of 17 days: however, detection of viral RNA does not necessarily equate to infectiousness and viral culture has been rarely positive beyond nine days of illness.
reference
BMJ 2020;371:m3862 http://dx.doi.org/10.1136/bmj.m3862 Published: 23 October 2020
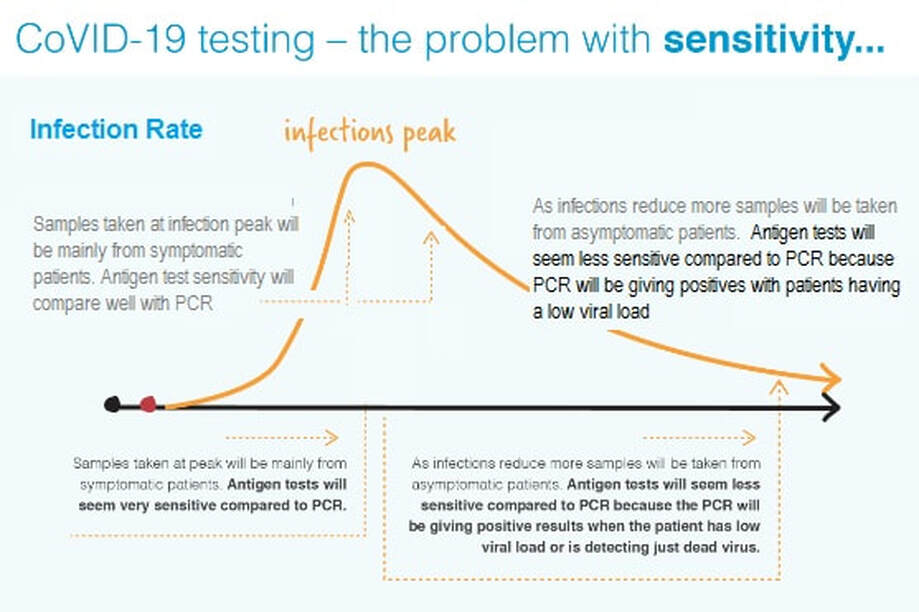
Infection rates affect measurements of test accuracy – Sensitivity parameter becomes meaningless, or worse, misleading
Antigen tests are known to operate at high viral loads whilst PCR can give positives at both high and low viral loads. If the evaluation of an Antigen test against PCR is done when infection rates are high most samples submitted to the laboratory will be from symptomatic patients – the antigen test and PCR test will be looking at patients with a high viral load so the Antigen test will have a high sensitivity.
However, as the infection rate slows down more samples will be submitted from asymptomatic or recovering patients with lower viral loads. Whist these may give positive results with PCR they will give negative results with Antigen tests; hence the Antigen test will have a low sensitivity.
The sensitivity of an Antigen test against PCR is meaningless unless the viral load is specified.
references
https://www.bmj.com/content/369/bmj.m1808
https://reflectionsipc.com/2020/05/21/screening-patients-and-staff-without-symptoms-for-sars-cov-2-beware-false-positives-and-negatives/#more-4560
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30453-7/fulltext
Antigen tests are known to operate at high viral loads whilst PCR can give positives at both high and low viral loads. If the evaluation of an Antigen test against PCR is done when infection rates are high most samples submitted to the laboratory will be from symptomatic patients – the antigen test and PCR test will be looking at patients with a high viral load so the Antigen test will have a high sensitivity.
However, as the infection rate slows down more samples will be submitted from asymptomatic or recovering patients with lower viral loads. Whist these may give positive results with PCR they will give negative results with Antigen tests; hence the Antigen test will have a low sensitivity.
The sensitivity of an Antigen test against PCR is meaningless unless the viral load is specified.
references
https://www.bmj.com/content/369/bmj.m1808
https://reflectionsipc.com/2020/05/21/screening-patients-and-staff-without-symptoms-for-sars-cov-2-beware-false-positives-and-negatives/#more-4560
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30453-7/fulltext
Viral Load correlates with infectiousness and symptoms
It takes live virus to cause an infection. The initial quantity of virus will be small but as the infection takes hold the virus numbers will increase (viral load) slowly, then rapidly, and symptoms will occur. As the patients recover, viral load will decrease. Both virus and virus particles will continue to be detectable for a time after the symptoms have subsided.
The two methods of testing for the virus are PCR and Antigen. PCR can give positive results with a low virus load whilst the Antigen tests require a high virus load.
PCR detection of viruses is helpful so long as its accuracy can be understood; it offers the capacity to detect RNA in minute quantities, but is this viral RNA active? If the RNA detected is not from a live virus it is a false positive.
It is also important to realise a TRUE POSITIVE in PCR does not always mean that the person presents any danger to society. True positive results can occur after the patient ceases to be infective because the viral load is too low.
PCR testing is suitable for very large numbers of tests but requires significant amounts of expensive equipment which leads to centralisation of testing with inevitable delays.
Antigen methods are more suitable for limited numbers of on-site testing. However, it is becoming apparent that there is a correlation between high viral load, onset of symptoms and probability of infectiousness.
reference
https://www.cebm.net/study/duration-of-infectiousness-and-correlation-with-rt-pcr-cycle-threshold-values-in-cases-of-covid-19-in-england/
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30354-4/fulltext#%20
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa851/5865363
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa851/5865363
It takes live virus to cause an infection. The initial quantity of virus will be small but as the infection takes hold the virus numbers will increase (viral load) slowly, then rapidly, and symptoms will occur. As the patients recover, viral load will decrease. Both virus and virus particles will continue to be detectable for a time after the symptoms have subsided.
The two methods of testing for the virus are PCR and Antigen. PCR can give positive results with a low virus load whilst the Antigen tests require a high virus load.
PCR detection of viruses is helpful so long as its accuracy can be understood; it offers the capacity to detect RNA in minute quantities, but is this viral RNA active? If the RNA detected is not from a live virus it is a false positive.
It is also important to realise a TRUE POSITIVE in PCR does not always mean that the person presents any danger to society. True positive results can occur after the patient ceases to be infective because the viral load is too low.
PCR testing is suitable for very large numbers of tests but requires significant amounts of expensive equipment which leads to centralisation of testing with inevitable delays.
Antigen methods are more suitable for limited numbers of on-site testing. However, it is becoming apparent that there is a correlation between high viral load, onset of symptoms and probability of infectiousness.
reference
https://www.cebm.net/study/duration-of-infectiousness-and-correlation-with-rt-pcr-cycle-threshold-values-in-cases-of-covid-19-in-england/
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30354-4/fulltext#%20
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa851/5865363
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa851/5865363
30 minute Antigen Test - no equipment required

Multi Target Antibody test - higher sensitivity


